Slipping rib syndrome (SRS) is a frequently overlooked cause of persistent chest wall, rib, flank, and upper abdominal pain. Many patients spend months or even years searching for answers because standard imaging tests such as X-rays, CT scans, and MRIs often appear entirely normal.
At Barr Center for Innovative Pain & Regenerative Therapies, we evaluate patients with chronic rib and chest wall pain from a structural and functional perspective. Once properly identified, slipping rib syndrome can often be treated effectively using targeted regenerative therapies such as prolotherapy.
What Is Slipping Rib Syndrome?
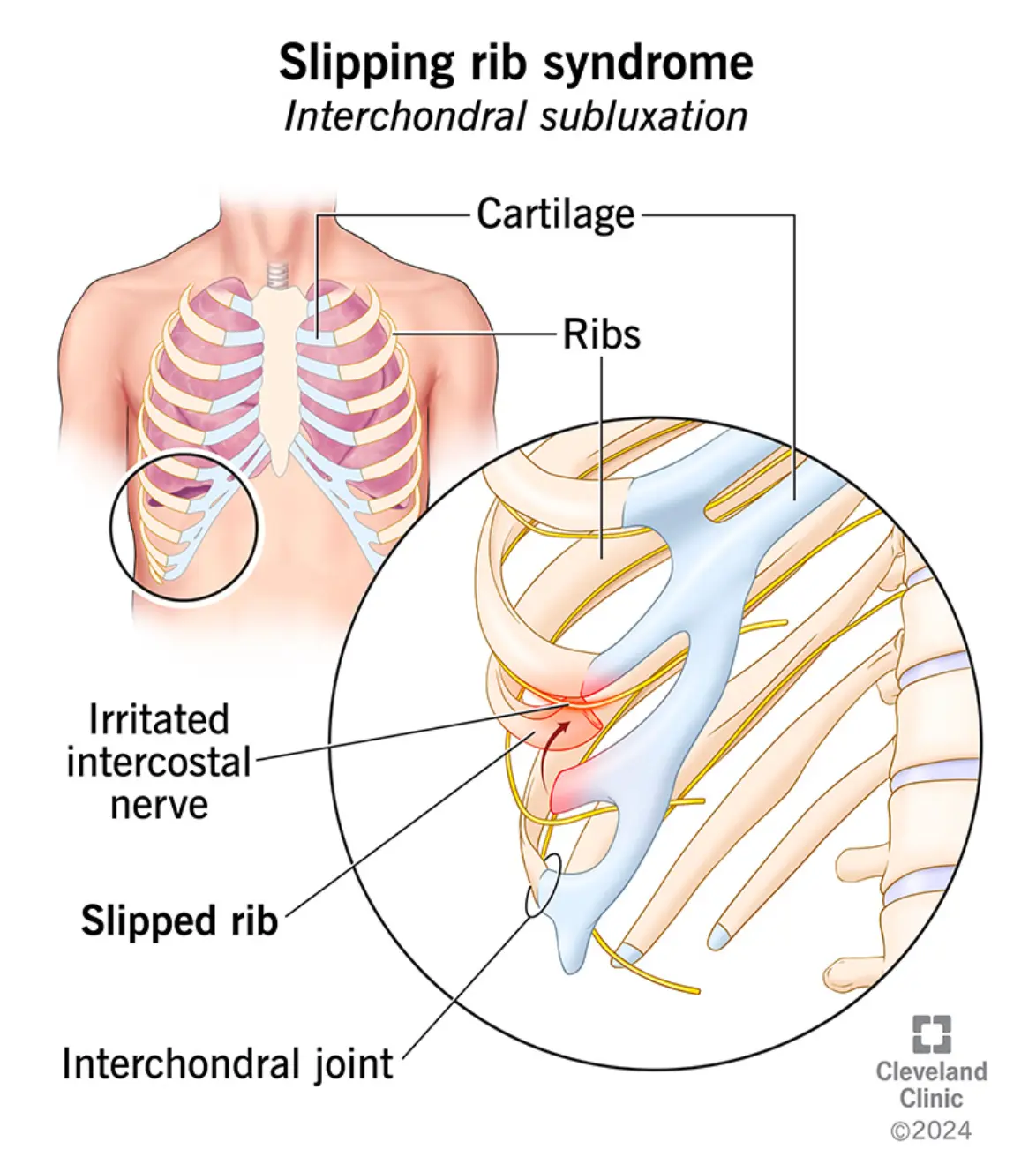
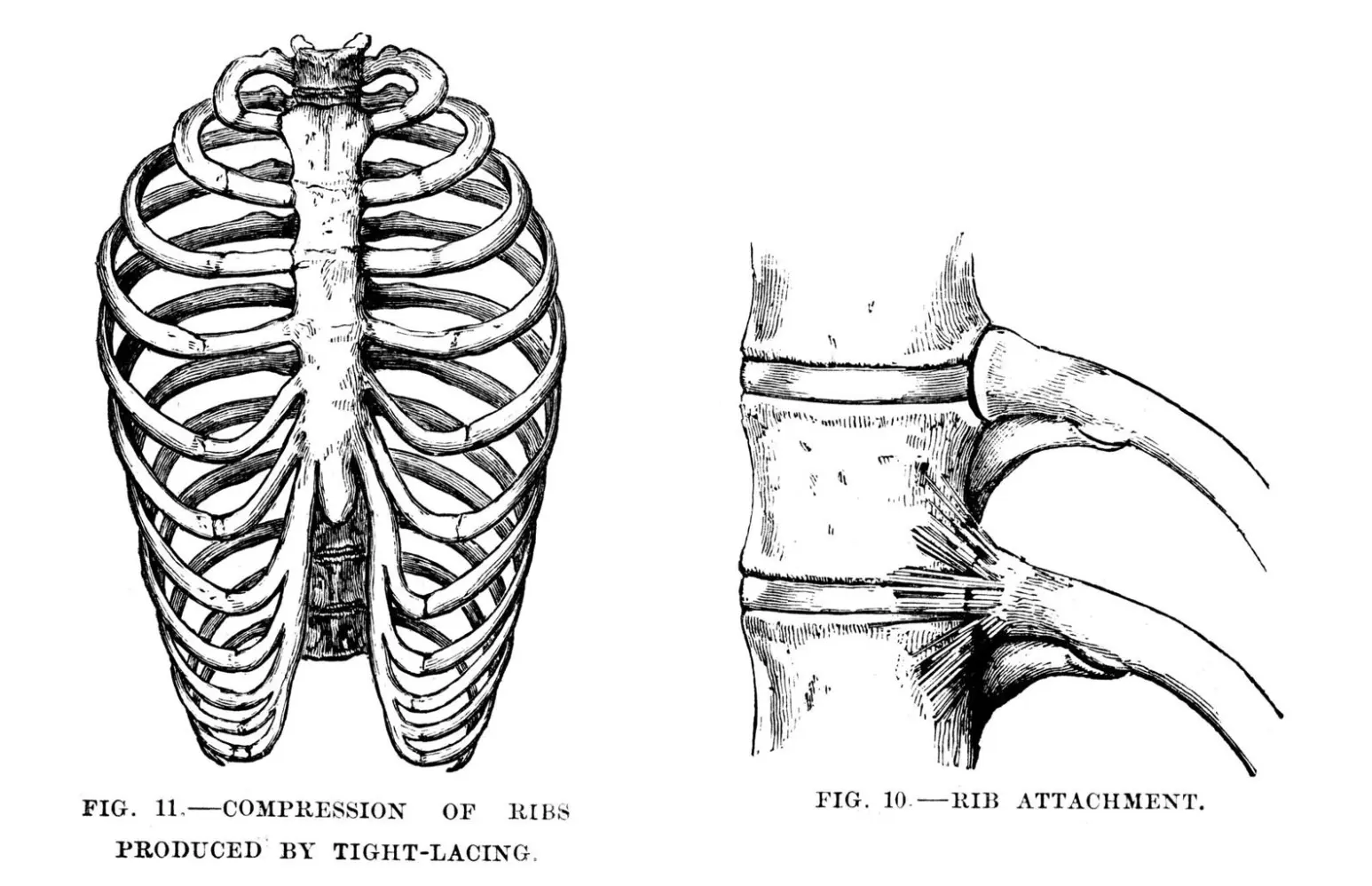
Slipping rib syndrome occurs when one of the lower ribs, most commonly ribs 8, 9, or 10, becomes excessively mobile due to weakened or injured ligaments that stabilize the rib cage. These are called false ribs because, unlike the upper ribs, they attach to the sternum indirectly through cartilage rather than directly.
When the supporting ligaments loosen or sustain injury, the affected rib may:
- Partially sublux, or shift out of position
- Slide beneath the adjacent rib above it
- Irritate nearby intercostal nerves
This nerve irritation produces the characteristic, often sharp and episodic pain associated with the condition. Although first described over a century ago, slipping rib syndrome remains underdiagnosed in modern clinical practice. It has also been called Cyriax syndrome, rib tip syndrome, and clicking rib syndrome.
Clinical definition: Slipping rib syndrome is a condition in which the lower ribs become hypermobile due to ligament laxity, allowing the rib to shift or sublux and irritate nearby intercostal nerves, causing chest, rib, or upper abdominal pain.
Anatomy of the Rib Cage
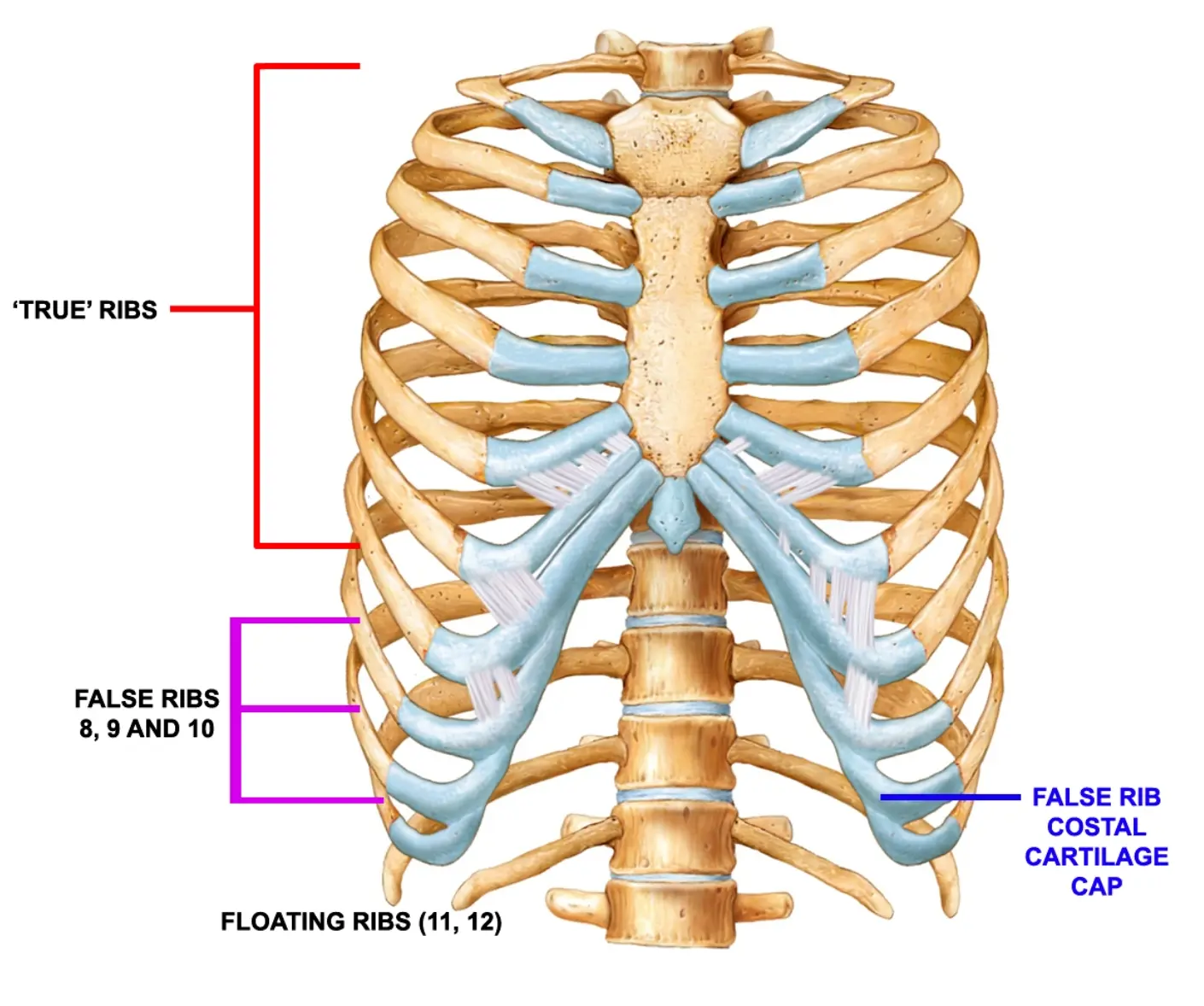
The human rib cage contains 12 pairs of ribs, categorized into three groups:
- True ribs (1-7) – attach directly to the sternum via costal cartilage
- False ribs (8-10) – attach indirectly to the sternum through the cartilage of the rib above and form the costal margin
- Floating ribs (11-12) – do not attach to the sternum
Slipping rib syndrome most commonly involves false ribs, particularly ribs 8 through 10. These ribs depend heavily on ligamentous and cartilaginous connections for stability. The intercostal nerves run along the inferior border of each rib. When a rib shifts or subluxes, it may compress or irritate these nerves, producing the condition’s characteristic pain patterns.
Causes and Risk Factors
Several factors can contribute to ligament laxity and rib instability:
Trauma
Direct trauma is one of the most common triggers. Examples include falls, motor vehicle accidents, contact sports injuries, and blunt chest trauma. Even minor trauma can stretch the interchondral ligaments enough to cause lasting instability.
Repetitive Motion
Activities involving repetitive twisting or rotational movements can gradually strain rib attachments. This includes golf, tennis, baseball, rowing, and yoga. Over time, this cumulative strain may lead to ligament laxity.
Hypermobility and Connective Tissue Laxity
Patients with generalized joint hypermobility or connective tissue laxity are more prone to rib instability. Hormonal changes that increase ligament flexibility, including those during pregnancy, can also be a contributing factor.
Chronic Cough
Prolonged coughing places repeated stress on rib attachments. Common causes include chronic bronchitis, asthma, and post-viral cough.
Symptoms of Slipping Rib Syndrome
Symptoms vary from person to person but often follow a recognizable pattern. Because they can closely mimic other conditions, patients are frequently evaluated for gallbladder disease, gastritis or GERD, kidney stones, costochondritis, intercostal neuralgia, and cardiac conditions before a correct diagnosis is reached.
Common symptoms include:
- Sharp or stabbing pain in the lower chest or upper abdomen
- A clicking, popping, or slipping sensation in the ribs
- Pain that worsens with twisting, bending, deep breathing, coughing, or sneezing
- Intermittent episodes rather than constant pain
- Pain that radiates to the back or flank
- Tenderness along the lower rib margin
Many patients describe a persistent feeling that a rib is popping out of place. Because standard imaging studies frequently appear normal, patients may be told that nothing is wrong or that the pain is muscular or stress-related. In reality, the cause is often mechanical instability of the rib cage.
Diagnosis
Diagnosis is primarily clinical, based on the patient’s history and physical examination. No single imaging study reliably confirms slipping rib syndrome, which is why thorough evaluation is essential.
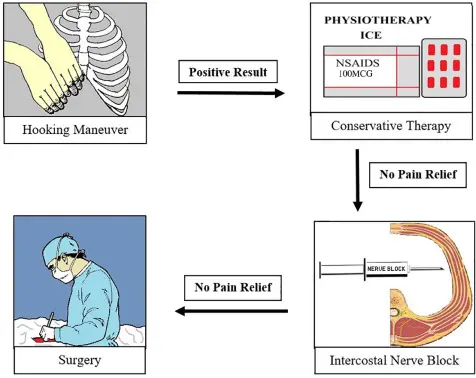
The Hooking Maneuver
One widely used diagnostic technique is the Hooking Maneuver, first described by Heinz and Zavala in 1977. The physician gently hooks fingers beneath the costal margin and lifts upward. If this reproduces the patient’s pain or creates a palpable rib movement, slipping rib syndrome is strongly suspected.
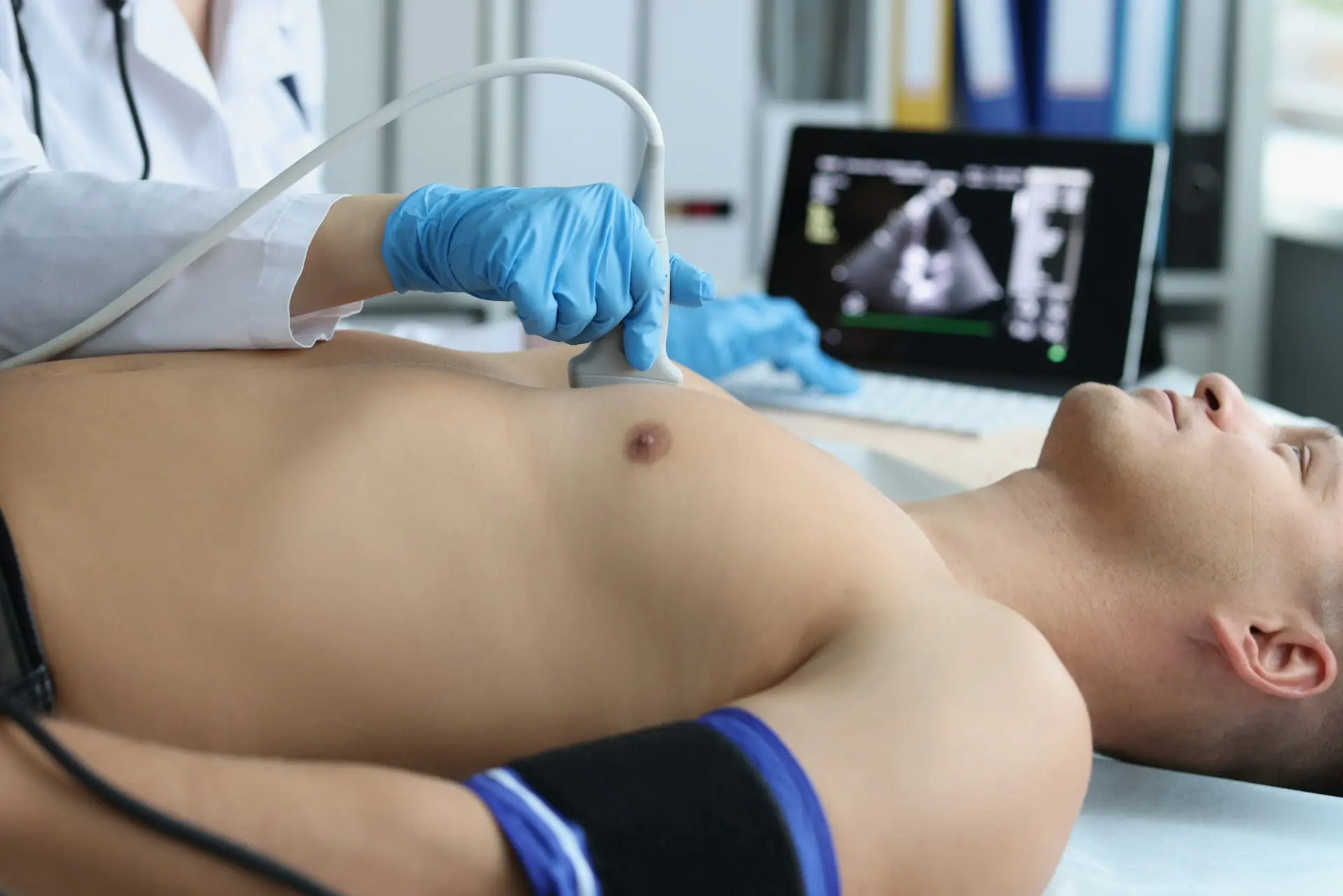
Musculoskeletal Ultrasound
At the Barr Center, we frequently use musculoskeletal ultrasound to evaluate rib instability. Unlike static imaging, dynamic ultrasound allows clinicians to observe rib movement in real time during examination. This makes it particularly valuable for identifying ligament injury and guiding both diagnostic and therapeutic injections.
Because X-rays, CT scans, and MRIs often appear normal in slipping rib syndrome, clinical examination, including the Hooking Maneuver and dynamic ultrasound, is the cornerstone of accurate diagnosis.
Conventional Treatment Options
Traditional treatments focus primarily on symptom management rather than correcting the underlying instability:
- Rest and activity modification
- Anti-inflammatory medications (NSAIDs)
- Rib belts or bracing
- Physical therapy, including core stabilization, thoracic mobility, and postural correction
- Intercostal nerve blocks to temporarily reduce nerve irritation
While these approaches can provide relief, they often do not address the root cause: ligament laxity and structural instability. In severe cases that fail conservative treatment, surgery may be considered, including rib stabilization or costal cartilage excision. Surgery is typically reserved for patients with persistent, debilitating symptoms who have not responded to other measures.
Regenerative Treatment: Prolotherapy
At Barr Center for Innovative Pain & Regenerative Therapies, we frequently treat slipping rib syndrome using prolotherapy, a regenerative injection therapy specifically designed to strengthen ligaments and stabilize joints.
What Is Prolotherapy?
Prolotherapy involves injecting a natural solution, commonly hypertonic dextrose, into weakened or injured ligaments. This stimulates a controlled healing response that promotes tissue repair.
The treatment works by:
- Activating fibroblasts, the cells that produce connective tissue
- Increasing collagen synthesis
- Strengthening the ligaments that stabilize the ribs
- Improving overall joint stability
Over time, this can help reduce rib hypermobility and decrease intercostal nerve irritation. Several published studies support the use of prolotherapy for chronic musculoskeletal ligament injuries.
Benefits of Prolotherapy for Slipping Rib Syndrome
When performed properly, prolotherapy may:
- Improve rib stability and reduce subluxation
- Decrease intercostal nerve irritation
- Relieve chronic rib, chest, and upper abdominal pain
- Improve breathing comfort
- Restore normal movement patterns
- Reduce or eliminate the need for surgery
Most patients undergo a series of treatments spaced several weeks apart, with gradual improvement over the course of care.
The Importance of Ultrasound-Guided Injections
The rib cage contains delicate structures including intercostal nerves, blood vessels, and pleural tissue. Precision is therefore critical. At the Barr Center, we use musculoskeletal ultrasound guidance to:
- Visualize the rib and costal cartilage in real time
- Identify specific areas of ligament injury
- Avoid nearby nerves and blood vessels
- Deliver regenerative injections with maximum accuracy
Ultrasound guidance improves both the safety and effectiveness of treatment.
Who Is a Good Candidate?
You may be a candidate for evaluation and regenerative treatment if you experience:
- Persistent rib, chest, or upper abdominal pain
- A clicking, popping, or slipping sensation in the ribs
- Pain triggered by twisting, bending, deep breathing, or movement
- Normal imaging results despite ongoing symptoms
- Limited or temporary relief from conventional treatments
A thorough evaluation is necessary to confirm the diagnosis and determine the most appropriate treatment plan for your individual situation.
Prognosis
The prognosis for slipping rib syndrome varies depending on the severity of ligament instability. Mild cases may improve with conservative care and activity modification alone. Chronic cases involving significant ligament laxity typically require targeted treatment to address the underlying mechanical cause.
When properly diagnosed and treated, many patients experience meaningful and lasting improvement in their symptoms. The goal at the Barr Center is to restore structural stability, not simply to mask pain, so that patients can return to normal activity and quality of life.
Frequently Asked Questions
Is slipping rib syndrome dangerous?
No. While it can be painful and disruptive to daily life, it is generally not life-threatening. Proper diagnosis is still important because symptoms can closely mimic other conditions.
Does it show up on MRI or CT?
Often it does not. Standard imaging frequently appears normal. Diagnosis relies primarily on clinical examination and dynamic ultrasound rather than static imaging.
How many prolotherapy treatments are needed?
Most patients require 3 to 6 treatments, spaced approximately 4 to 6 weeks apart, depending on the degree of ligament instability and individual response.
Is prolotherapy painful?
Most patients tolerate the injections well. Local anesthetic is typically used to improve comfort during the procedure.
Can it cause abdominal pain?
Yes. Because the lower ribs lie near the abdomen, pain can radiate and mimic gastrointestinal conditions such as gallbladder disease or gastritis.
Can it heal on its own?
In mild cases, symptoms may improve with rest. However, chronic cases involving ligament laxity typically persist unless the underlying instability is directly addressed.
References
- Foye PM. Slipping rib syndrome: an underrecognized cause of chest and abdominal pain. Pain Physician. 2012.
- Heinz GJ, Zavala DC. Slipping rib syndrome: diagnosis using the hooking maneuver. JAMA. 1977.
- Rabago D, Reeves KD, Doherty MP, et al. Prolotherapy for chronic musculoskeletal pain. American Journal of Physical Medicine & Rehabilitation. 2010.
- Cyriax J. On various conditions that may simulate visceral disease. Lancet. 1919.
Barr Center for Innovative Pain & Regenerative Therapies – Virginia Beach, VA
If you are experiencing persistent rib, chest, or upper abdominal pain that has not responded to conventional treatments, a comprehensive evaluation may help identify whether slipping rib syndrome is the cause.