At Barr Center for Innovative Pain & Regenerative Therapies, we frequently see patients who have been told for years:
- “All your imaging is normal.”
- “You’re just flexible.”
- “It’s anxiety.”
- “Nothing is wrong.”
Yet they live with persistent pain, joint instability, fatigue, and recurrent injuries. Often, the missing piece is hypermobility syndrome, including hypermobile Ehlers-Danlos syndrome (hEDS) or Hypermobility Spectrum Disorder (HSD). This blog explains how we approach diagnosis and treatment differently. 

Understanding Hypermobility
Hypermobility means joints move beyond the normal range. While flexibility can be advantageous in athletes and dancers, pathologic hypermobility can cause:
- Joint instability
- Frequent sprains or subluxations
- Chronic pain and muscle spasm
- Early degeneration of discs and joints
- Autonomic symptoms like POTS
- Fatigue and poor recovery
- MCAS
Over time, unstable joints overload surrounding tissues, including tendons, ligaments, fascia, and nerves. The problem is not too much flexibility. The problem is insufficient stability and poor connective tissue integrity.
How We Diagnose Hypermobility Syndromes
Diagnosis requires listening carefully and looking beyond imaging.
Clinical History
We assess:
- Recurrent sprains or joint “giving out”
- Childhood flexibility or being “double-jointed”
- Chronic tendonitis
- Family history of hypermobility
- Easy bruising or slow healing
- Dysautonomia symptoms such as lightheadedness or palpitations
- GI or mast cell issues
Many patients have seen multiple specialists before this pattern is recognized.
Physical Examination
We perform:
- Beighton score assessment
- Ligament stress testing
- Functional stability assessment
- Core and scapular stability testing
- Gait and movement analysis
- Assessment of breathing patterns and core muscle function
- Evaluation for embodied PTSD or reverse breathing patterns when relevant
The Beighton score is helpful, but it is not enough by itself. Some patients lose flexibility with age yet remain unstable.
Musculoskeletal Ultrasound and Bending X-Rays of the Back and Neck
We frequently use diagnostic ultrasound to evaluate:
- Ligament laxity
- Tendon degeneration
- Micro-tears
- Effusions
- Joint capsule thinning
Ultrasound allows dynamic assessment, which is something MRI often misses. Motion X-rays of the spine help assess underlying ligament laxity and micro-instability that can contribute to chronic myofascial pain.
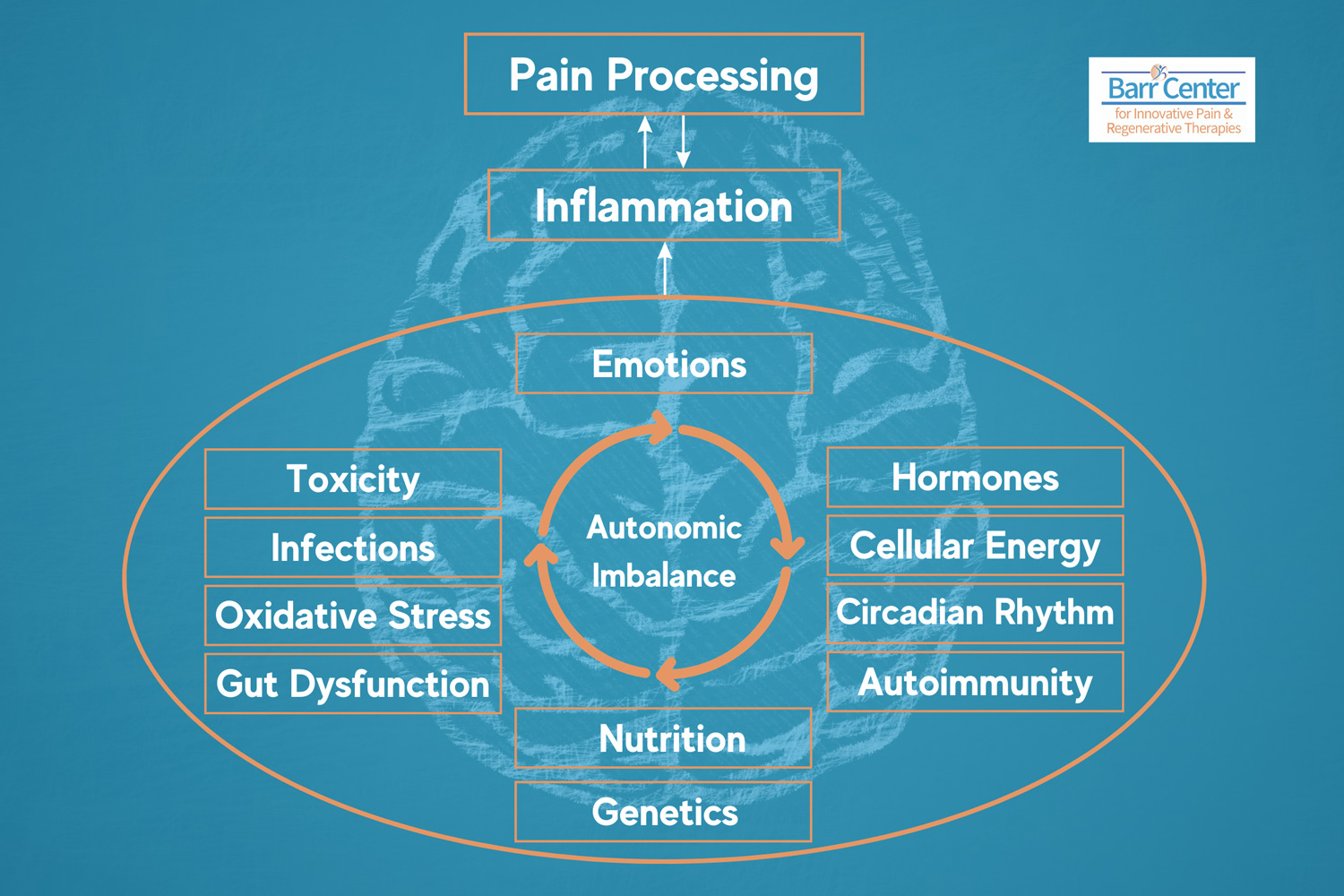
Root Cause Evaluation
Hypermobility is rarely isolated. We assess:
- Inflammation patterns
- Hormonal influences, since estrogen can affect ligament laxity
- Nutrient status, including vitamin C, copper, zinc, methylated B vitamins, and collagen cofactors
- Mitochondrial health
- Autonomic nervous system balance
- Other connective tissue disorders when appropriate
This whole-body approach is critical.
How We Treat Hypermobility at Barr Center
There is no one-injection solution. Treatment requires stabilization, regeneration, and nervous system retraining.
Targeted Regenerative Injections
These treatments are not covered by health insurance. We may use:
- PRP (platelet-rich plasma)
- Orthobiologics
- Prolotherapy
- Precision-guided ligament injections
These treatments aim to:
- Improve collagen signaling
- Strengthen ligament integrity
- Reduce micro-instability
The goal is not just pain reduction. It is structural stability restoration.
Stability-Focused Rehabilitation
Traditional physical therapy may overstretch hypermobile patients. We emphasize:
- Closed-chain strengthening
- Muscle re-education
- PRI and postural re-education
- Proprioceptive retraining
- Scapular stabilization
- Core activation
- Low-load, high-control movement
The objective is to teach the nervous system to better protect the joints.
Autonomic Nervous System Regulation
Many hypermobile patients experience dysautonomia. We incorporate:
- Breathing retraining
- HRV optimization
- Gradual conditioning protocols
- Stress modulation techniques
Stability improves when the nervous system is better regulated.
Connective Tissue Support
We optimize:
- Protein intake
- Collagen support
- Micronutrients involved in collagen synthesis
- Anti-inflammatory strategies such as low-dose naltrexone (LDN)
- Peptides that may support healing, improve muscle development, and reduce inflammation
Tissue quality matters.
Hormonal Considerations
Ligament laxity may fluctuate with hormonal shifts. We evaluate:
- Perimenopause
- Estrogen dominance
- Cycle-related symptom patterns
Stability can change dramatically across life stages.
Why Early Diagnosis Matters
Undiagnosed hypermobility can lead to:
- Early osteoarthritis
- Recurrent surgeries
- Chronic opioid use
- Central sensitization
- Loss of athletic identity
Proper identification can change the trajectory.
Our Philosophy
At Barr Center, we view hypermobility syndromes not as a limitation, but as a stability challenge that can often be improved with precision care. We combine:
- Advanced diagnostics
- Regenerative therapies and peptides
- Neuromuscular retraining
- Functional medicine insights
The result is a personalized stabilization strategy.
Common Questions
Is hypermobility curable?
No, but symptoms can often improve significantly with structured stabilization and regenerative support.
Is surgery helpful?
Surgery may fail in hypermobile patients if the underlying instability is not addressed.
Can regenerative medicine help?
In properly selected patients, yes, particularly for ligamentous laxity and chronic tendon overload. If you or someone you love has chronic joint instability, unexplained musculoskeletal pain, or has been told “everything looks normal,” we invite you to explore a deeper evaluation. Stability is strength, and strength can be rebuilt.